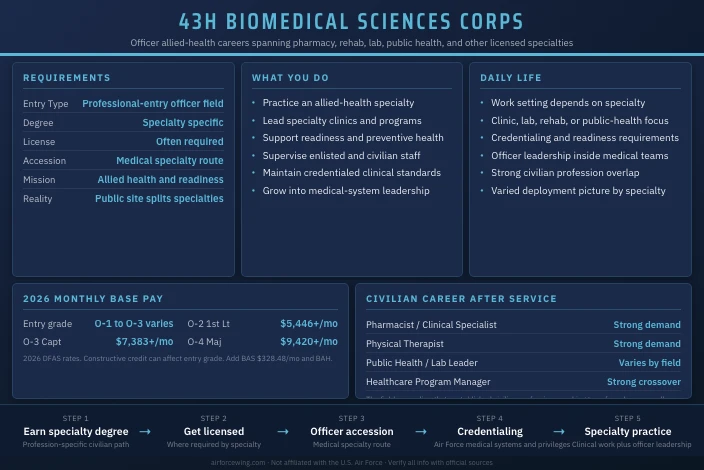
43H Biomedical Sciences Corps Officer
Some Air Force medical officers are physicians. Some are nurses. The rest of the medical system still needs serious licensed professionals: pharmacists, physical therapists, audiologists, optometrists, biomedical laboratory leaders, public-health officers, and more. This site uses 43H Biomedical Sciences Corps as the practical umbrella label for that allied-health officer lane. Current public recruiting pages usually break the corps into specialty-specific families instead of one single landing page, so this profile is intentionally broader than a one-specialty AFSC page.
If you are comparing this against a standard officer-accession route, the AFOQT study guide is useful background before you dive into medical specialty recruiting.
Job Role
43H Biomedical Sciences Corps officers are licensed allied-health professionals who practice their specialty inside the Air Force medical system while also serving as commissioned officers. Depending on specialty, they may run pharmacy services, rehabilitation programs, laboratory operations, public-health programs, or other clinical and preventive-health functions critical to force readiness.
Corps Breadth
This is one of the broadest officer communities in Air Force medicine. The day-to-day work depends on the specialty you bring with you. A pharmacist, physical therapist, and public-health officer are all serving the same medical enterprise, but they are solving very different problems.
Public-Source Context
The public healthcare careers pages usually list these jobs separately rather than under one combined corps page. Examples include bioenvironmental engineering, public health, pharmacy-adjacent roles, and other clinical specialties. This page uses 43H as a reader-friendly corps-level label so applicants can compare it against 44X, 46N, and 48X.
| Corps-Level Label On This Site | Public Recruiting Reality |
|---|---|
| 43H Biomedical Sciences Corps | Multiple specialty-specific healthcare officer pages |
| One comparison page | Several professional-entry tracks with distinct degrees and licenses |
Mission Contribution
The corps fills the spaces physicians and nurses do not cover alone. Medication safety, rehabilitation, preventive health, specialty diagnostics, and professional allied-health leadership all sit inside this mission set. The force is healthier and more deployable because these officers exist.
Salary
Officer Base Pay
2026 compensation follows the DFAS military pay tables.
| Rank | Grade | Typical YOS | Monthly Base Pay |
|---|---|---|---|
| Second Lieutenant | O-1 | Under 2 | $4,150 |
| First Lieutenant | O-2 | 2-4 years | $5,446-$6,485 |
| Captain | O-3 | 4-10 years | $7,383-$8,376 |
| Major | O-4 | 10-16 years | $9,420-$10,402 |
Many specialty officers receive constructive credit that affects entry grade. Exact rank depends on the profession, degree level, and current accession policy.
Allowances And Benefits
- BAH: location based
- BAS: $328.48 monthly
- TRICARE Prime
- BRS retirement and TSP matching
Civilian Value
The civilian transfer value is excellent because these officers are already practicing real professions that exist outside the military.
Qualifications
Specialty-Dependent Entry Standards
This field is only broad at the corps level. Entry requirements are specific at the profession level.
| Specialty Example | Typical Baseline |
|---|---|
| Pharmacist | PharmD and license |
| Physical Therapist | DPT or qualifying PT degree and license |
| Audiologist / Optometrist | Specialty doctorate and license |
| Public Health / Bioenvironmental / Lab roles | Degree and credential requirements vary by specialty |
The current Air Force healthcare pages are the right place to verify profession-specific requirements because they publish those tracks separately instead of under one 43H page.
Accession Reality
This is primarily a professional-entry field. Candidates are usually already trained or far along in their profession before the Air Force commissions them. That is why the best way to think about 43H is not “Which test score gets me in?” but “Which licensed specialty am I bringing into the service?”
Still, if you are comparing a direct medical commission against a general officer package, the AFOQT study guide helps frame the broader officer-accession picture.
Upon Commissioning
New officers enter with clinical expertise in a specialty, but they still need to learn how that specialty works inside the Air Force medical system. Military credentialing, readiness requirements, and officer leadership are the early growth areas.
Work Environment
Setting And Schedule
Because the corps is broad, the work environment varies by specialty. Some officers are in clinics. Some are in hospitals. Some are in labs, rehabilitation programs, public-health offices, or preventive-medicine environments. The common thread is that you are practicing a licensed health profession inside a military system that cares deeply about readiness.
Officer-NCO Dynamic
The medical environment is collaborative. These officers work with enlisted technicians, civilian specialists, nurses, physicians, and administrators. Leadership is less about parade-ground formality and more about clinical credibility, communication, and responsibility.
Corps Flexibility
The upside of a broad corps is variety. A long career may include clinical practice, education, program leadership, and higher-level medical staff work, depending on specialty.
Training
Training Pipeline
| Phase | Location | Length | Focus |
|---|---|---|---|
| Professional degree and licensure | Civilian university and boards | Specialty dependent | Become fully qualified in your profession |
| Officer accession training | Maxwell AFB or specialty accession path | Verify current length | Military officership and Air Force integration |
| Medical orientation / credentialing | Duty station | 1-8 weeks | Air Force systems and privileges |
| Specialty mission seasoning | Unit of assignment | 12-24 months | Clinical practice and officer leadership |
The public recruiting site gives this community in pieces rather than one combined path. That means course names and lengths vary by specialty. Candidates should verify the exact current accession training path with a Health Professions Recruiter.
If you are still weighing medical direct commission against a standard accession route, the AFOQT study guide gives the broader officer context.
Additional Development
This corps rewards specialty excellence first, then leadership. The officers who rise are the ones who stay technically credible while also learning how medical units really function.
Career Progression
Timeline
| Rank | Grade | Typical Timeline | Development Focus |
|---|---|---|---|
| Entry-grade specialty officer | O-1 to O-3 depending credit | Entry | Practice specialty and learn Air Force systems |
| Captain | O-3 | Early career | Section leadership and program ownership |
| Major | O-4 | Mid-career | Department-level leadership or staff roles |
| Lieutenant Colonel | O-5 | Senior career stage | Senior clinical or administrative leadership |
| Colonel | O-6 | Highest corps leadership track | Medical-group and enterprise roles |
Promotion Drivers
Clinical credibility, readiness, and leadership in your specialty matter more than generic resume-building. The Air Force needs allied-health officers who are genuinely good at the profession they brought into uniform.
Broadening
This field can open doors into education, policy, medical readiness, research-adjacent work, and higher headquarters medical staff roles.
Physical Demands
Fitness Standards
43H officers take the standard Air Force Fitness Assessment.
| Component | Max Points |
|---|---|
| 1.5-mile run | 60 |
| Push-ups | 10 |
| Sit-ups | 10 |
| Waist or body composition | 20 |
Beyond that, the physical demand depends on the specialty. A rehab or field-public-health role feels different from a lab-based specialty, even though both are in the same broader corps.
Deployment
Deployment Tempo
Deployment tempo varies sharply by specialty. Some roles deploy regularly in support of medical readiness. Others are more home-station focused. The corps-level answer is that deployment is possible, but the exact operational rhythm is profession dependent.
Duty Stations
Most assignments follow major medical facilities, medical groups, and specialized mission units that need a particular profession. The corps offers decent geographic variety, but not every specialty exists at every base.
Risk/Safety
Main Risks
The risk profile is professional and operational rather than mechanical:
- Clinical decision-making in specialized care
- Readiness accountability for deployable populations
- Burnout from high-demand healthcare fields
- Scope-of-practice errors when leadership gets sloppy
Control Measures
The corps depends on licensure, credentialing, peer review, and disciplined clinical practice. Good officers also stay honest about what is and is not inside their scope.
Impact on Family
Family impact depends heavily on specialty and assignment. Some tracks are stable clinic jobs. Others carry more deployment, call, or readiness burden. The good news is that the civilian career overlap is usually strong, which makes long-term family planning easier than in some narrower military-only fields.
Reserve and Air National Guard
Component Availability
Reserve-component opportunities exist, but they vary by specialty and unit demand. Applicants should treat component availability as profession specific rather than assuming every allied-health field is evenly distributed across Active Duty, Guard, and Reserve.
Civilian Integration
This is one of the best officer communities for civilian integration because the military work sits directly on top of already established civilian professions.
Post-Service
Civilian Career Paths
| Civilian Role | Typical Direction |
|---|---|
| Pharmacist / Clinical Specialist | Hospital, retail, federal, or specialty practice |
| Physical Therapist / Rehab Leader | Outpatient, sports, orthopedic, or hospital practice |
| Public Health / Lab Leader | Government, hospital, and analytic environments |
| Healthcare Program Manager | Clinical operations and administration |
Is This a Good Job
43H is a strong fit if you already want a licensed allied-health profession and want to practice it in a military system with real readiness consequences. It is a weak fit if you are still vague about the profession itself. The career starts with the license, not with the uniform.
More Information
- Review the Air Force Healthcare careers page for the current specialty-specific officer menu
- Review an example specialty page such as Bioenvironmental Engineer to see how the public site breaks this corps into separate tracks
- If you are still comparing commissioning routes, use the AFOQT study guide
This site is not affiliated with the U.S. Air Force or any government agency. Verify all information with official Air Force sources before making enlistment or career decisions.
Explore more Air Force medical officer careers and compare the physician lane at 44X Medical Officer or the nursing side at 46N Flight Nurse.