42G Physician Assistant
Air Force Physician Assistants are often the only provider in the room. At a remote operating location, on a special operations task force, or in a base clinic with 3,000 patients and no physician available that afternoon, a 42G officer diagnoses, treats, prescribes, and decides, with minimal oversight and maximum responsibility. This is not a supporting role.
The 42G AFSC sits in the Biomedical Sciences Corps and serves across family medicine, emergency care, orthopedics, occupational health, and operational medicine. Many PAs deploy as the primary provider for a deployed unit, serving alongside special operations forces or in austere locations where a flight surgeon is not present. The clinical experience that builds in three to four years of Air Force PA practice is difficult to replicate in civilian primary care.
If you’re finishing a PA program and wondering whether military medicine fits you, or if you’re an experienced PA looking at service as a second chapter, this guide covers the commissioning process, pay, training, and what the job actually looks like day to day.
Preparing for commissioning starts with understanding the officer selection process, the OTS preparation guide is a good starting point for the academic and fitness standards you’ll need to meet.
Job Role and Responsibilities
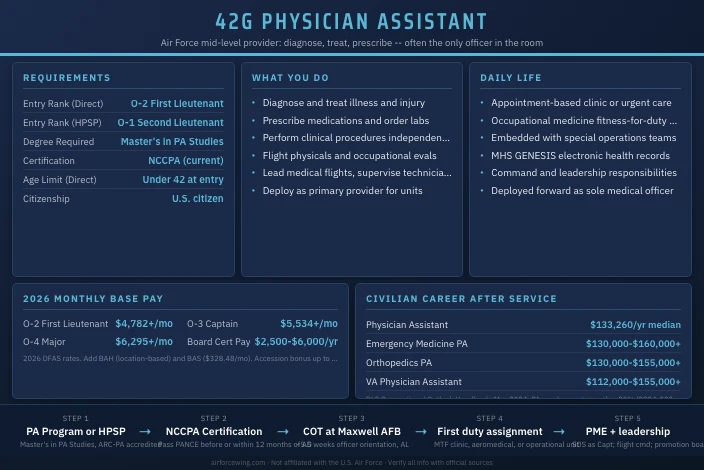
Air Force Physician Assistants (AFSC 42G) are commissioned officers in the Biomedical Sciences Corps who provide mid-level medical care across the full spectrum of Air Force operations. They diagnose and treat illness and injury, prescribe medications, order and interpret diagnostic tests, perform procedures, and manage patient care, operating under general physician supervision but with considerable independent authority in most duty environments. In deployed and operational settings, the 42G is frequently the senior medical officer present.
Command and Leadership Scope
At the flight level, a 42G PA typically leads a small clinical team: technicians, medical assistants, and in some cases junior officers. As a senior captain or major, a PA can serve as the medical director for a smaller medical unit or as a flight commander in a medical squadron. A lieutenant colonel with the right experience can lead a medical flight or serve in a group-level medical leadership role.
Span of control varies widely by assignment. A PA embedded with a special operations unit may have two or three enlisted medical technicians. A PA running a family practice flight at a large installation may supervise a dozen staff members.
Specific Roles and Designations
| Designation | Description |
|---|---|
| 42G3 | Physician Assistant (core designator) |
| 42GX | Flight Surgeon-equivalent PA in aeromedical roles |
| SEI 457 | Special Operations Medical Provider |
| SEI 451 | Aeromedical roles (selected PAs embedded with aviation units) |
Most 42G officers carry the core 3-skill level throughout their career. Additional qualifications and Special Experience Identifiers distinguish PAs who complete aeromedical or special operations tracks.
Mission Contribution
Every deployable unit needs medical coverage. Physicians are in short supply relative to the force’s global footprint, so PAs fill that gap, at bases, on deployment, and embedded with units that require a medically qualified officer who can operate independently. Air Force PAs also contribute to joint operations: a 42G officer may support Army special operations, Marine expeditionary units, or coalition partners when mission requirements demand it.
Technology, Equipment, and Systems
Air Force PAs use the same electronic health record systems as the broader military health system, including MHS GENESIS. In clinical settings they work with diagnostic imaging, laboratory systems, and standard procedural equipment. In aeromedical roles they may conduct flight physicals and use aerospace-specific evaluation tools. In austere environments they work with whatever is in the aid bag.
Salary and Benefits
Base Pay
Base pay for a commissioned officer is set by grade and years of service. Most newly commissioned PAs enter at O-2 (First Lieutenant) if they hold a current NCCPA certification and are fully qualified at the time of commissioning. HPSP students who commission during PA school enter at O-1. For applicants pursuing OTS, early AFOQT study guide strengthens the commissioning package.
| Grade | Title | Entry Pay | 4 Years | 8 Years |
|---|---|---|---|---|
| O-1 | Second Lieutenant | $4,150/mo | $5,222/mo | N/A |
| O-2 | First Lieutenant | $4,782/mo | $6,485/mo | N/A |
| O-3 | Captain | $5,534/mo | $7,383/mo | $8,126/mo |
| O-4 | Major | $6,295/mo | $7,881/mo | $8,816/mo |
2026 DFAS pay rates. Verify current rates at dfas.mil.
Special Pays
Medical officers receive special pays that significantly increase total compensation. The three main categories for 42G PAs are:
- Variable Special Pay (VSP): All credentialed PAs receive VSP; the exact rate is set by statute and published annually by DoD.
- Board Certification Pay (BCP): PAs certified by the NCCPA receive an additional $2,500 to $6,000 per year, scaled by years of creditable service.
- Incentive Special Pay (ISP): Eligible PAs who are not in initial training may receive up to $75,000 per year in incentive special pay tied to a service agreement.
- Accession Bonuses: Qualified PAs can receive $37,500 for a 3-year agreement or $60,000 for a 4-year agreement at accession. Exact availability changes annually based on Air Force health professions staffing requirements; confirm current bonus availability with an Air Force health professions recruiter.
Housing, Food, and Healthcare
Officers receive BAH (Basic Allowance for Housing) based on their duty location, grade, and dependency status. A single O-3 at a CONUS installation typically sees BAH ranging from roughly $1,200 to over $2,000 per month depending on local housing costs. BAS (Basic Allowance for Subsistence) adds $328.48 per month for officers in 2026.
Healthcare through TRICARE Prime costs nothing for active duty members. Medical visits, prescriptions, and hospitalization are covered at zero cost. Dental care for active duty is also no cost at military treatment facilities.
Retirement and TSP
Officers who reach 20 years of service receive a pension worth 40% of their high-36 average basic pay under the Blended Retirement System. The government automatically contributes 1% of basic pay to the Thrift Savings Plan after 60 days of service, then matches member contributions up to 4%, for a total maximum government contribution of 5% of basic pay.
Work-Life Balance
Active duty officers receive 30 days of paid leave per year. Work tempo depends heavily on assignment. A PA at a large base clinic with adequate staffing may work standard duty hours most weeks. A PA deployed to a small operating location or embedded with a special operations unit faces a very different schedule. TDY (temporary duty) assignments and training exercises add travel requirements between deployments.
Qualifications and Eligibility
Commissioning Paths
There are two main routes to a 42G commission: the Health Professions Scholarship Program (HPSP) and direct accession as a fully qualified PA.
Most Air Force PAs commission through one of these two paths. Traditional OTS and ROTC are not the primary routes for this AFSC; professional credentialing requirements make direct accession the norm for experienced PAs.
| Path | Who It’s For | Entry Rank | When You Commission |
|---|---|---|---|
| HPSP | Students enrolled in an accredited PA master’s program | O-1 (2d Lt) | During PA school (after 1st or 2nd year) |
| Direct Accession (Fully Qualified) | Credentialed PAs with current NCCPA certification | O-2 (1st Lt) | Before entry on active duty |
| ANG/Reserve Direct Commission | Licensed PAs seeking part-time service | O-2 (1st Lt) | Varies by unit vacancy |
HPSP covers tuition, fees, and a monthly stipend for up to 36 months while you complete your PA program. In exchange, you incur an active duty service commitment: typically one year of active duty for each year of scholarship support, with a minimum obligation. Students attend a Commissioned Officer Training (COT) course after their first or second year of PA school.
Direct accession is for PAs who already hold their degree and NCCPA certification. You apply between November and July; a board meets in early October. Qualified applicants commission directly, then proceed to COT before their first assignment.
Minimum Requirements
| Requirement | HPSP Track | Fully Qualified Track |
|---|---|---|
| Degree | Enrolled in accredited MPA/MPAS program | Master’s in PA Studies (accredited program) |
| Certification | NCCPA required within 12 months of active duty | Current NCCPA certification required |
| Age at entry | Under 39 at program completion | Under 42 at entry on active duty |
| Citizenship | U.S. citizen | U.S. citizen |
| PA Program Accreditation | ARC-PA accredited program | ARC-PA accredited program |
Test Requirements
The AFOQT (Air Force Officer Qualifying Test) is required for officer candidates who commission through OTS. For direct commission medical officers, including most 42G applicants, the AFOQT requirement may be waived or not required depending on the commissioning path. Confirm current test requirements with an Air Force health professions recruiter since the process differs from the standard OTS pipeline.
There is no TBAS requirement for this AFSC. The OTS preparation guide covers AFOQT structure and scoring in detail for those who do need the test.
Assignment Process
Health professions officers do not go through the standard AFPC assignment process that other career fields use. After commissioning, new 42G officers are assigned based on Air Force Medical Service manning requirements and mission needs. You can submit preferences, but the needs of the medical force drive placement.
Cross-training into 42G from another AFSC later in a career is possible but uncommon. Most officers in this field enter through one of the two accession paths above.
Upon Commissioning
HPSP students enter at O-1 (Second Lieutenant). Fully qualified direct accession PAs enter at O-2 (First Lieutenant). The standard active duty service commitment for a direct commission is 3 years for an unsponsored commission. HPSP obligations are calculated separately based on years of scholarship received.
Work Environment
Daily Setting
Most 42G officers work in military treatment facilities (MTFs), the Air Force’s clinics and hospitals on base. A PA at a large installation like Travis AFB, Wright-Patterson AFB, or Keesler AFB works in a clinic environment with appointment-based care. A PA at a smaller base may run the only medical clinic serving the entire installation, which means a broader scope of practice and higher patient volume per provider.
Outside of clinical settings, 42G officers work in occupational medicine evaluating fitness for duty, in aviation medicine units conducting aircrew physicals, or deployed to forward operating locations where they’re the primary provider for a unit. The deployed environment strips away many clinical comforts but adds a type of medical authority that few civilian practice settings offer at a comparable career stage.
Officer-NCO Dynamic
Medical officers work closely with senior enlisted medical technicians, the 4N0X1 Aerospace Medical Technicians and their senior NCO supervisors. A good PA listens to the flight chief. Senior NCOs know the unit, the patients, and the administrative requirements that make a clinic function. The 42G officer sets clinical standards and makes medical decisions; the senior enlisted runs the day-to-day operations.
Staff vs. Clinical Roles
Early career PAs spend most of their time in direct patient care. As a major or lieutenant colonel, a 42G officer may shift toward medical squadron operations, medical group staff positions, or joint assignments. Staff roles involve less direct patient contact and more administrative, policy, and leadership work. Both tracks are available and both lead to colonel for the most competitive officers.
Job Satisfaction and Retention
Air Force PAs tend to have strong retention relative to other medical officer categories. Key factors that keep PAs in uniform:
- Guaranteed patient volume and broad scope of practice
- Special pays (ISP, BCP, accession bonuses) that close the civilian gap
- Strong post-service career prospects across clinical and administrative medicine
- 20-year retirement with pension and lifetime healthcare
Common reasons officers leave after their initial obligation include compensation gaps relative to civilian PA salaries in high-cost urban markets, and PCS frequency separating families from established civilian careers or schools.
Training and Skill Development
Pre-Commissioning Training
HPSP recipients commission during PA school and attend a short Commissioned Officer Training (COT) course at Maxwell AFB, AL, after their first or second year of the program. This is not the full 9.5-week OTS; it is an abbreviated military orientation course that covers Air Force customs, courtesies, and leadership basics. The OTS preparation guide is useful background if you plan to commission through the standard OTS pipeline rather than direct accession.
Fully qualified direct accession PAs attend COT after commissioning and before their first active duty assignment.
Initial Skills and Pipeline
| Phase | Location | Duration | Focus |
|---|---|---|---|
| PA Program (HPSP) | Accredited civilian program | ~2 years | Clinical PA education |
| IPAP Phase 1 | JBSA-Fort Sam Houston, TX | ~16 months | Didactic instruction |
| IPAP Phase 2 | Military treatment facilities | ~13 months | Clinical clerkships |
| COT | Maxwell AFB, AL | ~5.5 weeks | Officer training |
| First duty assignment | AFPC-assigned installation | Ongoing | Clinical practice + leadership |
Professional Military Education
All Air Force officers attend Squadron Officer School (SOS) as captains, either in-residence at Maxwell AFB or via correspondence. It covers leadership theory, military strategy, and communication skills. Air Command and Staff College (ACSC) is available to majors selected for that program, and Air War College (AWC) is for senior officers at the colonel level. PME completion is an important factor in promotion board review.
Specialized Training
Air Force PAs with interest in operational medicine can pursue:
- Special Operations Forces Medical Skills Development course at Hurlburt Field, FL, which trains PAs embedded with AFSOC units in prolonged casualty care and austere medical techniques
- Aeromedical training for PAs assigned to aviation units, coursework covers aerospace physiology and flight-related medical evaluation
- AFIT (Air Force Institute of Technology) programs for fully funded graduate education in healthcare administration, public health, or related fields
The Air Force funds graduate education for selected officers through AFIT. A 42G officer can complete a master’s in healthcare administration or public health on full military salary, with tuition covered, during a qualifying assignment.
Career Progression and Advancement
Promotion Timeline
| Grade | Title | Typical Time-In-Grade | Key Developmental Positions |
|---|---|---|---|
| O-2 | First Lieutenant | ~2 years | Direct patient care, clinical skills development |
| O-3 | Captain | ~4 years | Flight commander (medical flight), staff PA roles, operational assignments |
| O-4 | Major | ~5 years | Medical squadron operations officer, staff positions, joint assignments |
| O-5 | Lieutenant Colonel | ~5 years | Medical squadron commander (select), medical group deputy |
| O-6 | Colonel | Variable | Medical group commander, AF Medical Service staff |
O-1 through O-3 promotions are essentially time-in-grade for officers meeting minimum standards. O-4 (Major) is the first board-selected grade. Historically, around 80% of eligible captains promote to major; the selection rate tightens at O-5 and O-6.
Building a Competitive Record
A 42G officer who reaches O-5 or O-6 has typically done more than just practice medicine. The path to promotion at senior grades requires:
- At least one flight or squadron command position (or equivalent leadership role)
- Completed in-residence PME at the appropriate career stage
- A deployment or operational assignment that demonstrates performance in difficult conditions
- Strong Officer Performance Reports with stratified rankings from senior raters
- At least one broadening assignment outside the primary clinical role
Cross-Training and Broadening
Active duty 42G officers who want to transition out of clinical medicine can apply for broadening assignments: ROTC instructor tours, joint staff billets, Air Staff positions in Washington D.C., and international health specialist assignments working with allied military medical programs. These assignments generally do not carry a clinical practice requirement and are typically 2-3 year tours.
Lateral movement to a different health professions AFSC is possible but requires a new credentialing and training process, this is uncommon and not a standard career path.
Physical Demands and Medical Evaluations
Fitness Assessment
All Air Force officers, including 42G PAs, take the Air Force Fitness Assessment annually. Standards are age- and gender-normed and do not vary by AFSC.
| Component | Maximum Points | Passing Minimum (under 25) |
|---|---|---|
| 1.5-Mile Run | 60 | Varies by age/gender |
| Waist Circumference | 20 | Must meet standard |
| Push-Ups (1 min) | 10 | Varies by age/gender |
| Sit-Ups (1 min) | 10 | Varies by age/gender |
| Composite | 100 | 75 minimum |
Each component has its own minimum threshold, failing any single component means failing the assessment regardless of total score. Verify current standards at af.mil since the Air Force updates scoring periodically.
Medical Standards for Commissioning
42G officers must meet Air Force officer physical standards at accession. The requirements are consistent with other non-rated officer AFSCs. There is no flight physical requirement unless assigned to an aeromedical role. Officers must maintain medical readiness throughout their career, including up-to-date immunizations and physical exams.
Prior medical history is reviewed at MEPS and during the commissioning medical exam. Conditions that require extensive medication management or that affect clinical duty performance may be reviewed by a waiver board. Contact an Air Force health professions recruiter if you have questions about specific conditions.
Deployment and Duty Stations
Deployment Tempo
The Air Force deploys medical officers on a rotational basis through the Global Health Engagement and Expeditionary Medical Support programs. Deployment frequency for 42G PAs varies by career stage and assignment location. Officers assigned to smaller bases with thin medical staffing may deploy more frequently to fill critical medical coverage gaps. Officers embedded with special operations units can expect a higher deployment tempo than those at large installation clinics.
A typical deployment runs 4 to 6 months. Combat medicine support, humanitarian medical operations, and joint partner-nation training missions are all possibilities depending on current operational requirements.
Primary Duty Stations
42G PAs can be assigned to any installation with a medical treatment facility. Large bases with major medical centers tend to have the highest concentration:
- Keesler AFB, MS: Air Force Medical Readiness training hub
- Wright-Patterson AFB, OH: Wright-Patterson Medical Center, academic medicine
- Travis AFB, CA: David Grant USAF Medical Center, large patient population
- Joint Base San Antonio, TX: Largest Air Force medical concentration in CONUS
- Ramstein AB, Germany: Primary overseas medical hub in Europe
- Yokota AB, Japan: Pacific theater medical support
Officers assigned to special operations units will be at AFSOC installations including Hurlburt Field, FL, and overseas locations tied to AFSOC missions.
Assignment preferences are submitted through AFPC, but health professions manning requirements drive final placement. Join spouse policy can be applied but is not guaranteed.
Risk, Safety, and Legal Considerations
Job Hazards
Clinical and operational risks for 42G PAs fall into several categories:
- Patient safety risk: Diagnostic errors, medication errors, and procedural complications are the primary clinical hazards. PAs manage patients independently across multiple specialties, which increases the breadth of clinical decision-making compared to a narrowly specialized civilian role.
- Deployed environment hazards: Hostile environments, limited diagnostic resources, and the physical demands of caring for trauma patients in non-ideal conditions. PAs embedded with special operations units operate in the same environments as the units they support.
- Command accountability: A 42G officer who serves as a medical flight commander or higher is legally accountable for the operations and readiness of that unit. Poor command climate, resource management failures, or personnel actions can result in official reprimands or relief for cause, consequences that are career-ending.
Safety Protocols and Legal Framework
Air Force PAs practice under clinical privileges granted by the Medical Treatment Facility commander. Those privileges define scope of practice and are reviewed periodically. Key compliance frameworks include:
- Operational Risk Management (ORM): Applied to both clinical and operational decision-making
- UCMJ: All Air Force officers are subject to the Uniform Code of Military Justice governing professional conduct and command accountability
- Federal Tort Claims Act: Medical malpractice liability for care provided in a military capacity is generally covered under FTCA rather than exposing the individual officer to personal liability
- Clinical privilege review: Periodic reassessment of scope of practice by the MTF commander
Impact on Family and Personal Life
PCS Tempo
Officers typically PCS (permanent change of station) every 2-3 years. For medical officers, PCS frequency can be slightly lower than in some other career fields because retaining experienced clinicians at stable installations has some operational value. Still, plan for three to five moves over a 10-12 year career.
Key family support resources available at every installation:
- Airman and Family Readiness Center (A&FRC): Relocation support, spouse employment resources, childcare referrals, and financial counseling
- Key Spouse Program: Connects military families within a unit during deployments and TDY periods
- Military OneSource: Free counseling, legal assistance, and transition support regardless of location
- School Liaison Officer: Assists with enrollment, records transfer, and special education needs during PCS moves
Dual-Military Couples
The Air Force manages dual-military couples through join spouse policy, which makes a good-faith effort to co-locate spouses at the same installation or within reasonable commuting distance. For health professions officers, this can be more complicated because assignment decisions are made by a medical manning system separate from the standard AFPC process. Dual-military couples with two health professions officers often get co-located, but it’s not guaranteed and is increasingly difficult at small installations.
Deployments and Family Stability
A typical 4-6 month deployment disrupts household routines significantly. The A&FRC and unit Key Spouses provide support during those periods. Pre-deployment family readiness checklists, power of attorney preparation, and connecting with other families in the unit go a long way toward managing the stress of separation.
Reserve and Air National Guard
Component Availability
The 42G AFSC is available in both the Air Force Reserve and the Air National Guard. Reserve and Guard PA officers work at reserve medical units affiliated with military treatment facilities, or in medical squadrons attached to flying wings that require medical support.
Commissioning Paths
Reserve and Guard PAs commission through direct accession, the same NCCPA certification and master’s degree requirements apply. Some units also accept officers who commission through the HPSP with a Reserve component obligation instead of active duty. Contact your target unit’s medical officer recruiter for unit-specific requirements.
Active duty 42G officers who complete their ADSC can transfer to a Reserve or Guard unit, which allows continued service at a reduced commitment while pursuing a civilian PA career.
Commitment and Schedule
Standard Reserve commitment is one Unit Training Assembly (UTA) per month (typically a weekend) plus two weeks of Annual Tour per year. Some 42G Reserve positions require additional clinical days to maintain patient care currency and maintain clinical privileges at the affiliated MTF.
Part-Time Pay
| Component | Grade | Approximate Monthly Drill Pay (4 UTAs) |
|---|---|---|
| Air Force Reserve / ANG | O-3 (Capt) | ~$1,384/mo for 4 drill periods |
Drill pay is based on 1/30th of monthly base pay per drill period. An O-3 with 4 years of service earns approximately $7,383/mo on active duty base pay, making each drill period worth roughly $246. Multiply by 4 UTAs per month for an approximate monthly drill figure.
Benefits: Reserve vs. Active vs. Guard
| Feature | Active Duty | Air Force Reserve | Air National Guard |
|---|---|---|---|
| Monthly Pay | Full base pay + allowances | Drill pay only (unless mobilized) | Drill pay only (unless mobilized) |
| Healthcare | TRICARE Prime (free) | TRICARE Reserve Select (premium) | TRICARE Reserve Select or state coverage |
| Education | Full GI Bill, Tuition Assistance | Partial GI Bill eligibility; TA available | State tuition waivers vary; TA available |
| Retirement | 20-year active pension (high-36) | Points-based reserve retirement | Points-based reserve retirement |
| Deployment Tempo | Moderate to high | Low to moderate (mission-dependent) | Low to moderate (mission-dependent) |
| Command Opportunities | Yes, multiple pathways | Yes, at unit level | Yes, at unit level |
| Special Pays | Full medical special pays | Proportional during active service | Proportional during active service |
Civilian Career Integration
Reserve and Guard PA service pairs well with civilian clinical practice. Many 42G Reserve officers work in civilian emergency departments, urgent care clinics, or hospital systems during the week and complete their military obligation on weekends and annual tours. Employers in healthcare are generally familiar with USERRA protections, which require job reinstatement after deployments and prohibit discrimination based on military service.
Post-Service Opportunities
Transition to Civilian Practice
An Air Force PA who serves 6-10 years leaves with clinical experience that civilian programs rarely replicate, high-volume patient care, procedural proficiency, independent practice authority in austere settings, and leadership at a young career stage. That record opens doors.
Civilian programs that actively recruit former military PAs include Department of Veterans Affairs healthcare facilities, academic medical centers, and hospital systems with military affiliate programs. The Transition Assistance Program (TAP) at your installation and Hiring Our Heroes are two practical resources for the 12-18 months before separation.
Civilian Career Prospects
| Civilian Role | Median Annual Salary | Job Outlook (2024-2034) |
|---|---|---|
| Physician Assistant | $133,260 | +20% (much faster than average) |
| Emergency Medicine PA | $130,000-$160,000+ | Strong |
| Orthopedics PA | $130,000-$155,000+ | Strong |
| Occupational Medicine PA | $120,000-$145,000+ | Moderate |
| VA PA (federal) | $112,000-$155,000+ | Stable, veteran preference |
BLS Occupational Outlook Handbook, May 2024. Specialty ranges based on industry survey data.
The BLS projects 20% employment growth for PAs over the next decade, one of the fastest growth rates of any healthcare occupation. About 12,000 new PA positions are projected to open each year.
Graduate Education and Credentials
NCCPA certification transfers directly to civilian practice. Officers leaving active duty have full Post-9/11 GI Bill eligibility if they served the qualifying time. The GI Bill covers in-state tuition at public universities in full, or up to $29,920.95 per year at private institutions for the 2025-2026 academic year.
PAs who want to transition to physician-level practice use the GI Bill for pre-med coursework or graduate-level bridge programs. Some choose healthcare administration or public health master’s programs, both use AFIT-funded graduate education opportunities available while still serving.
Is This a Good Job for You? The Right (and Wrong) Fit
Ideal Candidate Profile
This career field fits people who want significant clinical autonomy at a relatively young career stage, are comfortable with geographic mobility, and value the military lifestyle enough to accept its tradeoffs. If you’re finishing a PA program and want to start your career with 3-4 years of high-volume, diverse patient care, without the financial pressure of civilian student loan repayment, the Air Force offer is hard to beat on a financial-to-experience basis.
The accession bonus, zero-cost healthcare, housing allowance, and special pays change the math compared to a starting civilian salary alone. Run the full compensation comparison before assuming civilian practice pays more at entry level.
Potential Challenges
The job is not for people who want to stay in one city, build a private practice, or specialize narrowly in a high-earning specialty like dermatology PA or plastic surgery. The Air Force needs generalists who can function across family medicine, occupational health, and emergency settings. Specialization happens later in a career, and not always on the officer’s preferred timeline.
Common friction points for 42G officers:
- PCS frequency: Every 2-3 years disrupts personal networks, spouse careers, and children’s schooling
- Generalist scope: Specialization is limited and timeline-dependent; the Air Force assigns you where they need a PA, not where you prefer to practice
- Call schedules: Under-manned installations can produce heavy on-call loads, particularly with limited physician coverage
- Deployment tempo: 4-6 month rotations disrupt household routines and clinical continuity
Officers with strong roots in a specific community often find the PCS cycle harder to manage over a 10-12 year career than they expected when they first signed.
Career and Lifestyle Alignment
If your goal is 20 years and a pension, the 42G path works well for competitive officers willing to embrace leadership roles beyond clinical practice. If you’re aiming for a 4-year tour to pay off student loans, build clinical experience, and transition to civilian practice, the financial and career return is strong on that timeline too. The Guard and Reserve path offers a third option: continue PA practice in civilian settings while maintaining military affiliation and building toward reserve retirement.
More Information
Talk to an Air Force health professions recruiter before applying, the 42G accession timeline, bonus availability, and HPSP seat counts change by fiscal year. The Air Force Accessions Center at afaccessionscenter.af.mil maintains current program announcements. For officers considering the OTS pathway or wanting to understand the academic standards used in officer selection, the OTS preparation guide covers the AFOQT and what selection boards look for.
This site is not affiliated with the U.S. Air Force or any government agency. Verify all information with official Air Force sources before making enlistment or career decisions.
Explore more Air Force medical officer careers such as the 44X Medical Officer and 43H Biomedical Sciences Corps.